If your knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities such as walking or climbing stairs. You may even begin to feel pain while you are sitting or lying down. If medications, changing your activity level, and using walking supports is no longer helpful, you may want to consider total knee replacement surgery.
In total knee replacement surgery, the parts of the bones that rub together are resurfaced with metal and plastic implants. Using special, precision instruments. Your surgeon will typically remove the damaged surfaces of all three bones. The replacement surfaces will then be fixed into place.

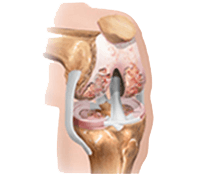
The knee is the largest joint in the body. Normal knee function is required to perform most everyday activities. The knee is made up of the lower end of the thigh bone (femur), which rotates on the upper end of the shin bone (tibia), and the kneecap (patella), which slides in a groove on the end of the femur. Large ligaments attach to the femur and tibia to provide stability. The long thigh muscles give the knee strength. The joint surfaces where these three bones touch are covered with articular cartilage, a smooth substance that cushions the bones and enables them to move easily. All remaining surfaces of the knee are covered by a thin, smooth tissue liner called the synovial membrane. This membrane releases a special fluid that lubricates the knee, reducing friction to nearly zero in a healthy knee. Normally, all of these components work in harmony. But disease or injury can disrupt this harmony, resulting in pain, muscle weakness, and reduced function.
Common Causes of Knee Pain and Loss of Knee Function
The most common cause of chronic knee pain and disability is arthritis. Osteoarthritis, rheumatoid arthritis, and traumatic arthritis are the most common forms. Osteoarthritis usually occurs in people 50 years of age and older and often in individuals with a family history of arthritis. The cartilage that cushions the bones of the knee softens and wears away. The bones then rub against one another, causing knee pain and stiffness. Rheumatoid arthritis is a disease in which the synovial membrane becomes thickened and inflamed, producing too much synovial fluid that overfills the joint space. This chronic inflammation can damage the cartilage and eventually cause cartilage loss, pain, and stiffness.
Traumatic arthritis can follow a serious knee injury. A knee fracture or severe tears of the knee ligaments may damage the articular cartilage over time, causing knee pain and limiting knee function.
Is Total Knee Replacement for you?
Whether to have total knee replacement surgery should be a cooperative decision made by you, your family, your family physician, and your orthopaedic surgeon. Your physician may refer you to an orthopaedic surgeon for a thorough evaluation to determine if you could benefit from this surgery. Alternatives to traditional total knee replacement surgery that your orthopaedic surgeon may discuss with you include a unicompartmental knee replacement or a minimally invasive knee replacement.
Reasons that you may benefit from total knee replacement commonly include:
- Severe knee pain that limits your everyday activities, including walking, climbing stairs, and getting in and out of chairs. You may find it hard to walk more than a few blocks without significant pain and you may need to use a cane or walker.
- Moderate or severe knee pain while resting, either day or night
- Chronic knee inflammation and swelling that does not improve with rest or medications.
- Knee deformity: a bowing in or out of your knee
- Knee stiffness: inability to bend and straighten your knee
- Failure to obtain pain relief from non-steroidal anti-inflammatory drugs. These medications, including aspirin and ibuprofen, often are most effective in the early stages of arthritis. Their effectiveness in controlling knee pain varies greatly from person to person. These drugs may become less effective for patients with severe arthritis.
- Inability to tolerate or complications from pain medications
- Failure to substantially improve with other treatments such as cortisone injections, physical therapy, or other surgeries
How A Knee Replacement Is Done?
You will most likely be admitted to the hospital on the day of your surgery. After admission, you will be evaluated by a member of the anesthesia team. We prefer spinal or epidural anesthesia, in which you are awake but your legs are anesthetized.The procedure itself takes approximately 2 hours. The damaged cartilage and bone will be removed and then the new joint is fixed to restore the alignment and function of your knee.
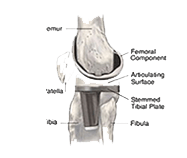
Many different types of designs and materials are currently used in total knee replacement surgery, nearly all of which consist of three components: the femoral component (made of a highly polished strong metal), the tibial component (made of a durable plastic often held in a metal tray/made of metal), and the patellar component (also plastic).
After surgery, you will be moved to the recovery room, where you will remain for 1 to 2 hours while your recovery from anesthesia is monitored. After you awaken, you will be taken to your hospital room.
Uni-compartmental Knee Replacement
Although not as common as total knee replacement, the partial or unicompartmental knee replacement (commonly called the “Uni”) is a viable alternative in limited situations. The designs of the unicompartmental types of knee replacements have improved over the years, as has the sophistication of the instruments used to implant these types of artificial joints. The unicompartmental knee replacement also has smaller, less invasive incisions. The unicompartmental knee replacement is used to replace a single compartment of the arthritic knee. The knee joint has three compartments: the medial (inner) compartment, the lateral (outer) compartment, and the patellofemoral (kneecap) compartment. If the damage is limited to either the medial or lateral compartment, that compartment may be replaced with the unicompartmental knee implant. If two or more compartments are damaged, unicompartmental knee replacement may not be the best option.
Unicompartmental knee replacement is also less desirable for a young, active person because it may not withstand the extremes of stress that high levels of activity create. It is best suited for the older, slim person with a relatively sedentary lifestyle. Only between 6 and 8 out of 100 patients with arthritic knees are good candidates for unicompartmental knee replacement. Because the unicompartmental knee replacement can be inserted through a relatively small incision (approximately 3 to 4 inches long), which does not interrupt the main muscle controlling the knee, rehabilitation is faster, hospitalization is shorter, and return to normal activities is more rapid than after a total knee replacement. However, this is still a serious surgical procedure, and has all of the same risks as total knee replacement. These risks, as well as whether you are a good candidate for unicompartmental knee replacement, should be discussed with your orthopaedic surgeon.
Minimally Invasive Knee Replacement
A recent advance in the performance of total knee replacement is the use of minimally invasive surgical approaches. This technique, still in its relative infancy, is more challenging than standard total knee replacement. The incisions are approximately half the size of those used in a standard approach. The smaller incisions and new techniques to expose the joint may result in short-term advantages such as a quicker rehabilitation, less pain, and a shorter hospitalization, according to some reports. The minimally invasive approach to the total knee replacement is appropriate for non-obese patients who have reasonable motion without significant deformity. Hospitalization may be reduced to 1 to 3 days among these patients, and the need for an extended stay for inpatient rehabilitation may be reduced or eliminated in most patients.
Why Knee Replacement Is Done?
Knee Replacement Surgery is recommended for people over the age of 50 with a stiff, painful knee that makes it difficult to perform even the simplest of activities usually due to osteoarthritis, rheumatoid arthritis or traumatic injuries and fractures.

What To Expect Before And After Surgery?
Once you and your surgeon decide that this surgery is right for you, a date will be scheduled for your surgery. Several things may be necessary to prepare for surgery. For example, your surgeon might ask you to have a physical examination by an M.D. Physician or your regular doctor. Because blood transfusions are likely to be needed during your surgery. you may want to donate one unit of your own blood or possibly two units if your surgeon feels it is needed. All preparations for surgery should be discussed with your surgeon. The average hospital stay is usually 4 days for knee replacement surgery. Almost all patients show a dramatic improvement within a month. Most people report a major reduction or no pain in the damaged joint once it is replaced by the artificial joint.
Recovery From Knee Replacement Surgery?
After knee joint replacement, many people are standing and moving the joint a day after the surgery. After about six weeks, most people are walking comfortably with minimal assistance. Once muscle strength is restored, people who have had knee joint replacement surgery can enjoy most activities except running and jumping.